The moderate aortic stenosis risk score is a new clinical tool designed to predict who is truly at risk of cardiac death or heart failure hospitalisation — and who is likely to do well. If you have been told you have moderate aortic stenosis, you have probably heard some version of “we’ll keep an eye on it.” For many patients, that is the right approach. But here is what we are learning: not everyone with moderate aortic stenosis faces the same outlook. Some patients remain stable for years. Others run into serious trouble well before their valve disease ever reaches the severe category.
As clinicians, we have known this for a while. A pooled meta-analysis of over 400,000 patients showed that moderate aortic stenosis carries around 2.5 times the hazard of cardiac death compared with mild or no valve disease. That is a number that should make us pay attention. But the harder question has always been: which patients are actually at risk, and which ones are going to do fine?
Why the current grading system falls short
Aortic stenosis is graded as mild, moderate, or severe based on echocardiographic measurements of the aortic valve. That framework is useful, but it treats everyone within the same severity band as though they carry equal risk. They do not.
A 60-year-old with moderate aortic stenosis, normal heart function, and no other cardiac issues is in a very different position from an 80-year-old with the same valve measurements but a weakened heart muscle, kidney disease, and a history of coronary artery disease. The valve looks the same on the echocardiogram. The risk does not.
Our earlier work, published in JACC: Cardiovascular Imaging, used unsupervised machine learning to identify four distinct phenotypes within the moderate aortic stenosis population: a low-risk group, a calcified aortic valve group, a low-flow group, and a cardiovascular-comorbid group. That study showed that comorbidities, not just the valve itself, are the main drivers of adverse outcomes. Importantly, the calcified aortic valve group appeared to derive the most benefit from valve replacement, while the low-flow group did not. These findings were externally validated in a geographically separate cohort.
That phenotyping work told us what kinds of patients exist within this population. The next step was to give clinicians a practical, quantifiable way to assess where a given patient sits on the risk spectrum.
Building a clinical risk score for moderate aortic stenosis
Our team developed and externally validated a clinical risk score to predict the 5-year risk of cardiac death or heart failure hospitalisation in patients with moderate aortic stenosis. The study was published in Echo Research & Practice in March 2026.
The derivation cohort included 2,212 patients from the Queensland Cardiac Outcomes Registry at Metro South Health in Brisbane, with a median follow-up of 4.3 years. The score was then validated in an independent cohort of 1,141 patients from Western Health in Melbourne, where echocardiographic parameters were manually validated by an experienced sonographer reviewing raw imaging data.
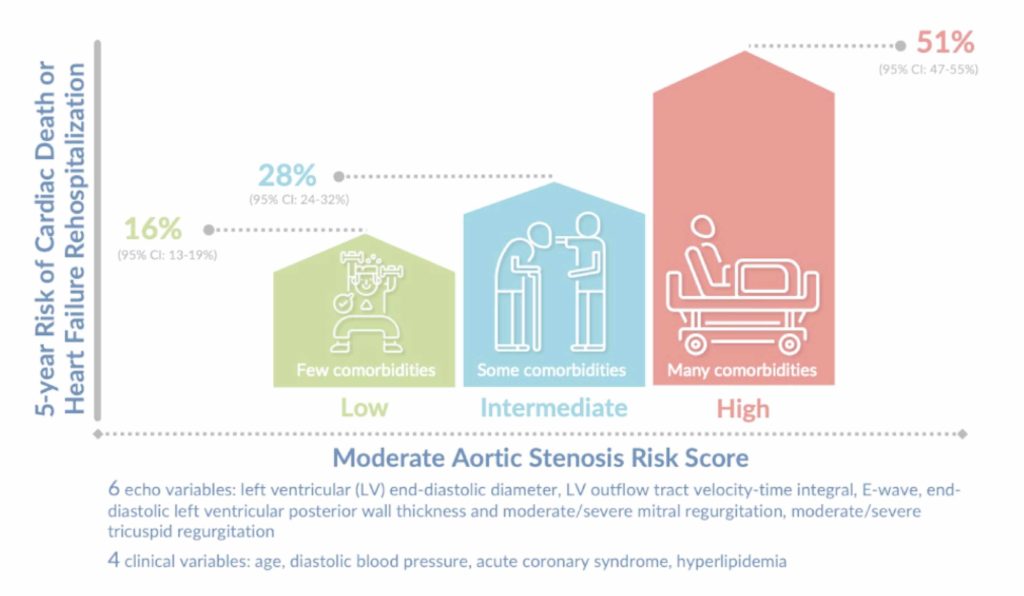
The final risk score uses 10 variables: six from a standard echocardiogram and four from the clinical history. These are data points most cardiologists already have at their fingertips during a routine consultation.
Echocardiographic variables (6)
- Left ventricular end-diastolic diameter
- Left ventricular outflow tract velocity-time integral
- Mitral valve E-wave velocity
- End-diastolic left ventricular posterior wall thickness
- Moderate or severe mitral regurgitation
- Moderate or severe tricuspid regurgitation
Clinical variables (4)
- Age
- Diastolic blood pressure
- History of acute coronary syndrome
- Hyperlipidaemia
Nothing exotic. No advanced imaging modalities, no genetic testing, no biomarkers that require special laboratory processing.
How well does it work?
The C-statistic for the composite outcome was 0.70 (95% CI: 0.67 to 0.76) in the internal validation dataset and 0.75 (95% CI: 0.70 to 0.79) in the external validation dataset. Time-dependent C-statistics across the five-year follow-up period ranged from 0.76 to 0.78 in the external cohort.
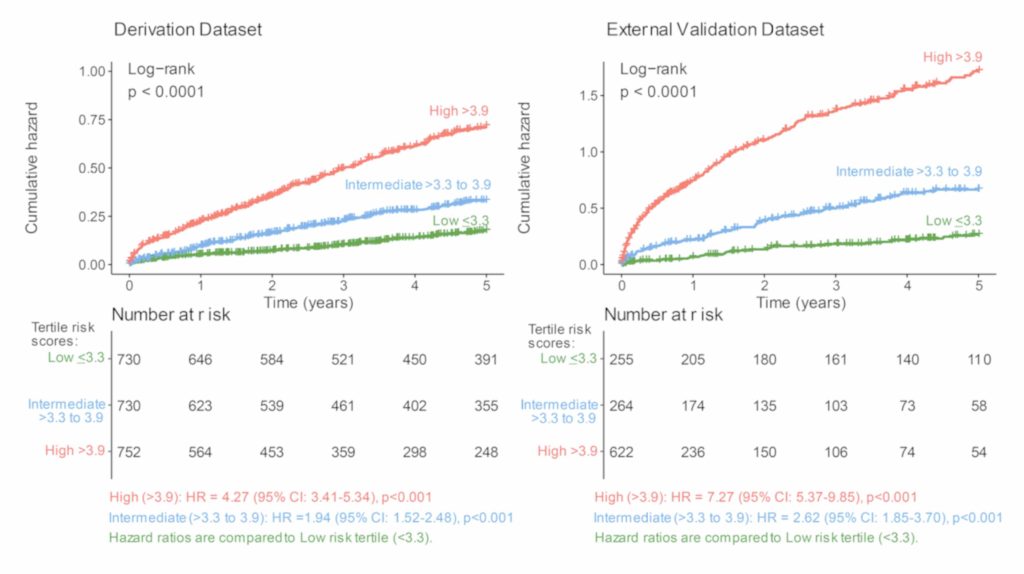
When patients were split into risk tertiles, the separation was clear. Patients in the highest-risk group (score greater than 3.9) had over four times the hazard of the composite outcome compared with the lowest-risk group in the derivation cohort (HR: 4.27, 95% CI: 3.41 to 5.34), and over seven times the hazard in the external validation cohort (HR: 7.27, 95% CI: 5.37 to 9.85).
Importantly, a sensitivity analysis showed that adding more variables beyond the top 10 did not meaningfully improve the model’s performance (C-statistic 0.76 in external validation with 17 variables versus 0.75 with 10). This supports the decision to keep the score parsimonious and clinically practical.
What does this mean for patients?
If you have moderate aortic stenosis, this does not change anything overnight. Your cardiologist is not going to rush you into surgery based on a risk score alone. But it adds an important piece to the conversation.
Until now, the discussion around moderate aortic stenosis has been somewhat binary: either you need an intervention (usually reserved for severe disease) or you do not. This score introduces nuance. It can help your cardiologist determine how closely you need to be monitored, how frequently you need imaging, and whether your overall cardiac health warrants a more proactive approach.
The bigger question: should we be intervening earlier?
There is an active debate in cardiology about whether some patients with moderate aortic stenosis might benefit from earlier valve replacement. Valve device companies are certainly keen on the idea, and randomised controlled trials such as the EXPAND TAVR II trial are underway. But even the most enthusiastic proponents would agree that replacing valves in everyone with moderate disease does not make sense.
The key is identifying the right patients. Observational data and our own phenotyping work suggest that early intervention may genuinely help a select subgroup, particularly those with calcified aortic valves. Our JACC Imaging study found that valve replacement was associated with reduced cardiac mortality in the calcified aortic valve phenotype, with this effect maintained after adjustment for surgical risk (adjusted HR: 0.28, 95% CI: 0.10 to 0.77 in external validation). However, the low-flow group showed no clear benefit, and in some analyses, intervention appeared to increase risk.
If trial evidence confirms that early intervention helps certain moderate aortic stenosis patients, a validated risk score becomes essential for identifying who stands to benefit rather than simply being exposed to procedural risk.
Try the moderate aortic stenosis risk score calculator
The moderate aortic stenosis risk score is designed as a decision-support tool. We have made the risk calculator freely available online. You can input the relevant clinical and echocardiographic variables and receive an estimated composite risk profile for conservative management.
Access the Moderate Aortic Stenosis Risk Calculator: https://baker-biostats.shinyapps.io/AS_risk_calculator/
It is designed as a decision-support tool, not a replacement for clinical judgement. The score is intended to inform discussions between clinician and patient, not to dictate management.
Read the full papers
Risk score paper (2026): Sen J, Salim A, Hakamuwa Lekamlage D, Wahi S, Marwick TH. Clinical risk score for cardiac death or heart failure hospitalization in moderate aortic stenosis. Echo Research & Practice. 2026;13:8. Open access
Phenotyping paper (2025): Sen J, Wahi S, Vollbon W, et al. Definition and Validation of Prognostic Phenotypes in Moderate Aortic Stenosis. JACC: Cardiovascular Imaging. 2025;18(2):133-149. Open access
Get in touch
If you have been diagnosed with moderate aortic stenosis and want your risk profile assessed as part of a comprehensive cardiac evaluation, or if you are a clinician interested in integrating this score into your practice, feel free to contact our rooms. Referring doctors can find referral information here.
Dr Jonathan Sen is a cardiologist and cardiovascular researcher based in Brisbane, Australia. He practices at Premier Cardiology at The Wesley Hospital, with subspecialty interests in cardio-oncology and valvular heart disease.